Based on these initial considerations, a study called “Farmaper” was run by the Italian Society of Hospital Pharmacies and Community based Pharmaceutical Services (SIFO), in collaboration with CERGAS at the SDA Bocconi School of Management. The aim of this research project was to lay the foundations for building a performance management system for the advancement of pharmacies and pharmacists in the INHS.
Specifically, we compiled two questionnaires to assess the degree of engagement of pharmacies and pharmacists, and the value produced within the sphere of the INHS. Actively participating in the survey were 70 public healthcare organizations (representing 35%) located homogeneously throughout the country.
What emerges from our analysis of the data is that today, INHS pharmacists play a major role in certain types of activities that don’t always correspond to what would be perceived as “high value added,” i.e. where the distinctive competencies of these professionals can “make a real difference.” Likewise, there are certain functions that take up their time and resources, despite the fact that these duties could be performed by other INHS staff.
How can we remap the geography of the activities undertaken by pharmacies and pharmacists? Answering that question means focusing on finding the best way to optimize the resources of healthcare organizations, especially now, at a time when the prospects for the industry are being redefined. The role of pharmacists, working in primary care, specialty services, acute and long-term care settings, is an essential one in light of their competencies: they sit on commissions evaluating pharmaceuticals and medical devices; they perform oversight and they serve as pharmacological watchdogs. Along with all this, other high-value-added functions can be found in at least 85% of the healthcare organizations we surveyed. Examples here include professional consulting linked to quality & risk management, in which the added-value of the pharmacists lies above all in patient-centric activities that tie into the appropriate use of both drugs and medical devices. The competencies of pharmacists also qualify them to lend a hand in budgeting processes, goal setting and resource allocation at an organizational level.
Our findings also shine a light on some areas where added value is high but the pharmacy structures of the healthcare organizations are not totally on board. For example, in the context of quality & risk management, ony 65% of the healthcare organizations in our sample offered training on quality and safety issues relevant to internal processes of pharmacies. Instead, areas where there is greater distance between the added value generated and the actual involvement of professional pharmacists is pharmacological reconnaissance and therapeutic reconciliation (both in local health authorities and in public hospitals). We saw the same for oversight aligning with current regulations which, despite the high value attributed to this activity by the pharmacists themselves, is done in a very small number of local health authorities (only one-third).
Among university teaching hospitals and institutes for treatment and research, there is room for improvement in embracing the antimicrobial stewardship function. In fact, despite the high value reflected by respondents, this activity is done in only 65% to 70% of the healthcare organizations in our survey.
Special consideration can be made for the logistical function as well. In this context, there are activities which are seen as high value added and very constructive for professional development. (For example, pharmacists are considered irreplaceable in managing therapy for rare or “orphan” diseases for which drugs are lacking; in coordinating, supervising and monitories logistics-related activities; and in providing specialist consulting when drawing up and assessing tender specifications for bids from pharmaceutical suppliers.) There are other types of activities as well that pharmacists perform in at least 85% of the healthcare organizations, both at a local level and in hospital settings (submitting requests for drug orders, handling orders for pharmaceuticals and medical devices, managing warehouse turnover), yet these are the sorts of jobs that could be delegated to other staff members.
In light of the pandemic, our investigation could not neglect a close examination of the specific role of pharmacists in dealing with the Covid-19 emergency. Respondents to our survey pointed out the capacity of pharmacists to produce value as far as the procurement and distribution of Personal Protective Equipment (PPE), the creation of professional networks, the production of galenic formulations specifically to address the needs of Covid-19 patients and support for clinics in general. By the same token, some other areas emerged as critical. A lack of tools and resources for procuring drugs and medical devices was one example. Also, better coordination and engagement would have been useful from pharmacists in healthcare organizations system wide, with clearer guidance at a local and regional level, and more of a voice in decision-making processes. In addition, there was no chance to consolidate competencies on safety and hygiene, topics that have become more critical than ever in recent months.
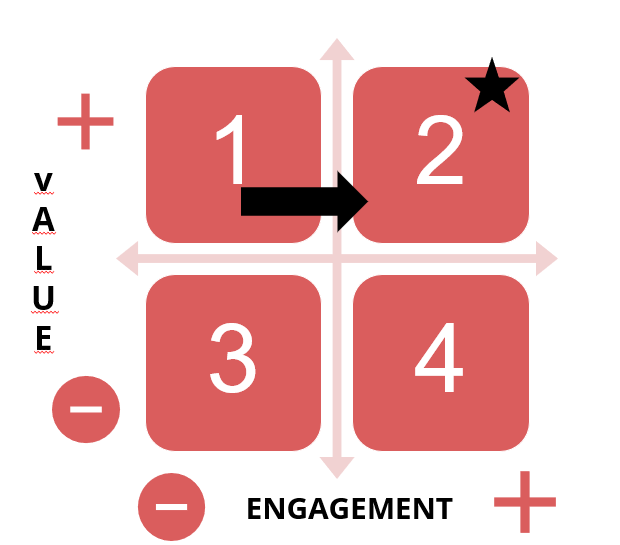
Figure 1 – Pharmacy services in local health authorities, teaching hospitals, university teaching hospitals and reaserch hoapitals: an evolutionary perspective






{kind=link}